
Two types of knowledge have shaped the path for the professionalisation of architecture and the contingent skills claimed by architects.
Occupational and professional powers are related to technical (i.e., the component transferable by standardisation and routinisation) and indeterminate (i.e., the non-transferable component, such as artistic initially inaccessible components of new research) elements of professional knowledge.
In architecture, technical aspects are adapted from engineering and technological fields, such as civil and mechanical engineering and computerised information.
The utilisation of technical knowledge is a significant source of income because it is an instrumental tool (e.g, BIM and CAD programmes) in carrying out architectural tasks, informed decisions and input in the early design process. Nonetheless, the progressively technical nature of professional knowledge dramatically develops de-professionalisation.
Therefore, technical aspects may unintentionally decrease professional autonomy. By contrast, the indeterminate components of professional practice, including aesthetics and generating new scientific knowledge, might permit architects to preserve some exclusive professional autonomy.
Aesthetics is scientific and non-transferable, as knowledge cannot support evidence-based design until it is produced and shared. These contributions are essential to the users, clients, and society.
However, there are concerns about architectural knowledge domains using knowledge formalisation.
Autonomy
Autonomy provides an analysis of the formation of the discipline of architectural design. ‘The Production of the Practical Knowledge’ is a constitutive component of a structure of occupational control.
The autonomy of the architect is bordered in all directions; the client controls the budget while the constructability is controlled by builders, engineers, and industry’s materials/equipment and is susceptible to economic conditions; architecture operates on conditions that can be easily doubted, its legitimating is obstinately cultural rather than compelling scientific, and issues of style are particularly outstanding.
It is defined as self-governance; in theory, professionals are equipped with the knowledge, extensive education and licenses. In architectural practice, autonomy is found when architects can make design decisions free from external constraints.
Architects need to become client-focused and entrepreneurial to win design commissions, leading to decreased artistic autonomy for practitioners since owners want to control their aesthetics. Thus, the conflict generated from the interaction between style, other design issues and different tastes among architects and lay people is defined as aesthetic complexity.
Specialised knowledge
With increasing project complexity and technological development, the specialised knowledge domains are more important than ever. Healthcare, due to its complexity, demands a range of knowledge and skills, including:
- Functional efficiency and design flexibility
- Technologies
- Medical knowledge of design
- The design impacts the behaviour and the psychological needs of the occupants
- Market and finance
- Future pandemics and risks
Holistic healthcare design complexities
Functional Complexity; due to operational issues since the design required three functional zones based on services:
- Medical services (e.g, medical ward, consulting clinics, emergency, radio-diagnostic, operating rooms / obstetric, and ICU/CCU/ laboratories)
- Medical support (e.g, pharmacy, sterile, library, records)
- General support (e.g, administration, food/linen supply and disposal, engineering/maintenance, transport and communication)
The change within these zones increases the complexity. For example, rapid developments in medical technology in the diagnosis and treatment departments change medical practice and demand modifications in functional relationships (e.g, the proximity of spaces). Therefore, the unprecedented requirements increase the hospital’s functional complexity and speciality.
Technological Complexity; the technology available at the construction time is another factor influencing healthcare design. Mechanical systems are a particular example; elevators and radiological technology have also influenced the form of hospitals as a critical component of modern hospital design. The most significant factor influencing modern medical practice is radiological technology with a significant impact and MRI.
Research (scientific knowledge) Complexity; knowledge plays a significant role in healthcare design and the most dramatic transformations in the field. Healthcare design has been affected by two scientific knowledge domains:
- A. Medical knowledge on the health outcomes of the patient
- B. Environmental psychology in response to the ‘supportive design’
The design is affectionate with medical knowledge and practice forms. Thus, all subsequent modifications to hospital design might be the product of alterations in medical knowledge. For example, hospital shapes (e.g, from block-plan to pavilions to skyscraper hospitals) present the impact.
The psychologists shaped current healthcare facility configurations and suggested that nature has a healing effect on patients. Therefore, the healthcare design will be more hospitable as the human touch, ‘supportive design’ become a focal point in healthcare architecture based on the quality-of-life experience; designing from a psychological perspective and promoting wellness via:
- A. Controllable physical and social surroundings
- B. Social support
- C. Positive distractions in physical surroundings
Aesthetic complexity; psychologists suggest that architects use a different system to understand and evaluate the environment than lay people.
This different system of judgment is implemented within the architectural schools during the period of education; the same implies that aesthetic appraisal could be different between architects and users due to their different backgrounds. Thus, this difference can cause conflicts associated with a design decision between clients/users and architects.
Architects and their artistry is the core skill in architectural design. Architecture has not established a monopoly over other aspects of building in professions like engineering, claiming expertness in building practice.
Thus, aesthetic theories have influenced architecture to secure its position in the building industry. Aesthetic theories (e.g, postmodernism, deconstructionism) have generated their own style. The rhetoric of style is a critical component of coherent aesthetic practice in organising professional status and constructing a market for professional services.
Interest Group Complexity; many interest groups, including funding agents, administrators, and doctors. This multi-voiced situation leads to conflicts. Politics in planning and consensus-building among a heterogeneous planning group determine the design process.
The architect’s role is not limited to problem-solving and aesthetic expression; instead, it needs the skill of consensus building to negotiate the different demands among different interest parties which challenge the architectural practice.
Conclusion
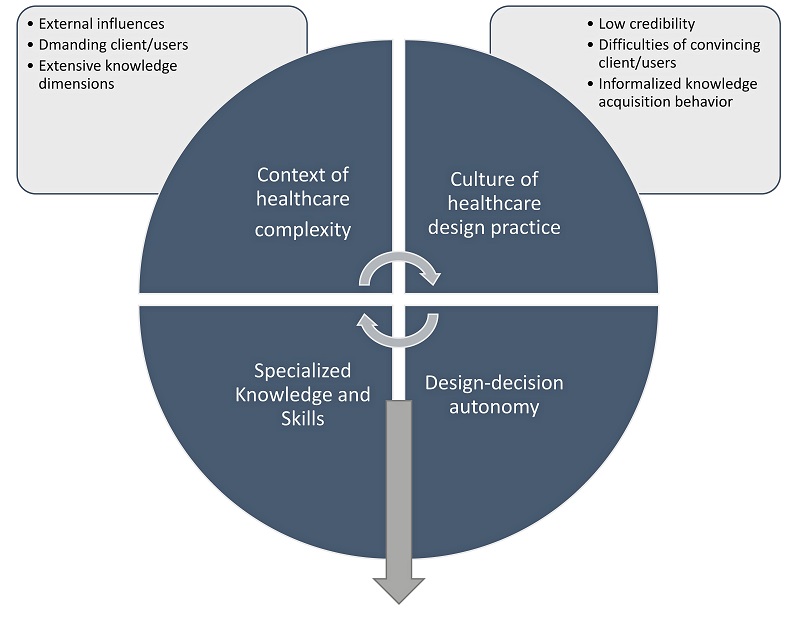
The context of healthcare design complexity appears to influence the culture of healthcare design practice. Likewise, changes in the culture of healthcare design practice may impact the context of holistic healthcare design complexity.
Increasing holistic healthcare design complexity may cause low credibility regarding the task performance of healthcare architects. Thus, increasing holistic design complexity decreases the design-decision autonomy of healthcare architects.
Specialised knowledge, including evidence-based design, may increase the design-decision autonomy of healthcare architects.
Healthcare design firms, which emphasise knowledge generation and evidence-based design, may increase the number of indeterminate elements of professional power. Consequently, this type of firm preserves design decision autonomy.
In summary, it’s always recommended that the complexity of healthcare design results from external influences, the demands of clients and users, and the need for extensive knowledge.
They experience difficulty convincing clients of their design decisions, and the informality of standard information acquisition (without research/scientific knowledge) is not fully respected.
Strong delivery is a dominant design philosophy of healthcare design firms. The context of healthcare design complexity includes external influences (e.g, regulatory issues, clients/users and healthcare policies).
Specialised knowledge domains (e.g, technical aspects, building systems, and indeterminate elements, such as artistry and unique knowledge generation through research) play a critical role in holistic healthcare design.
Another finding, clients/users of healthcare facilities are knowledgeable and specific about what they want. Architects struggle to persuade clients/users to accept their design decisions due partly to their lack of knowledge, which reverses the competence gap between professionals and clients. Consequently, architects perceive that their design-decision autonomy is decreasing.
It is always suggested that specialised knowledge and skills positively impact design-decision autonomy. Therefore, research-informed design decisions may increase the design-decision autonomy of healthcare architects.
The implication for the practitioner is that they will benefit greatly from the incorporation of research into the design process. Additionally, to support this process, universities should incorporate curricula in evidence-based design to prepare young architects to interpret and, ideally, conduct research.